


 Carpal Tunnel Syndrome (CTS) is a compression neuropathy, i.e. a pinching of the median nerve within the wrist.
Carpal Tunnel Syndrome (CTS) is a compression neuropathy, i.e. a pinching of the median nerve within the wrist.
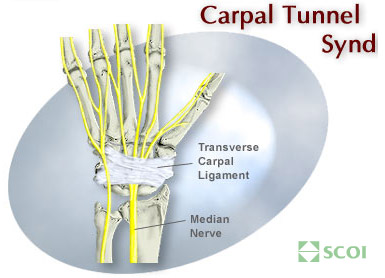
The carpal tunnel is a bony canal within the palm side aspect of the wrist that allows for the passage of the median nerve to the hand.
Pinching or compression of this nerve by the transverse carpal ligament sets into motion a progressively crippling disorder which eventually results in wrist pain, numbness and tingling in the hand, pain consisting of a “pins and needles” feeling at night, weakness in grip and a feeling of incoordination.
Who Gets CTS?
This disabling syndrome occurs more often in women than men, by a ratio of 3 to 1, usually between the ages of 30 and 50 years. Also, CTS is seen more frequently in people who tend to do forceful repetitive types of work, such as grocery store checkers, assembly line workers, meat packers, typist, accountants, writers, etc. Most patients generally visit their doctor with these complaints, and the diagnosis is confirmed after physical examination and appropriate nerve testing.
How is CTS Treated?
Treatment for CTS depends upon the stage of the disease. In the early stage, the syndrome can be reversible and is most often treated with appropriate modification in activities, a removable wrist brace, and anti-inflammatory medicines. In moderate stages of the disorder, especially if the numbness and pain continues in the wrist and hand, a cortisone injection into the carpal tunnel can be extremely beneficial. Surgical intervention in CTS is only indicated in those patients in whom non-operative treatment has failed to eliminate their symptoms. In patients with advanced disease, and especially in those who have profound weakness or muscle atrophy, surgical intervention should be done early. CTS should not be left untreated because it can eventually cause permanent nerve damage.
A common treatment of Carpal Tunnel Syndrome is a Carpal Tunnel Release:
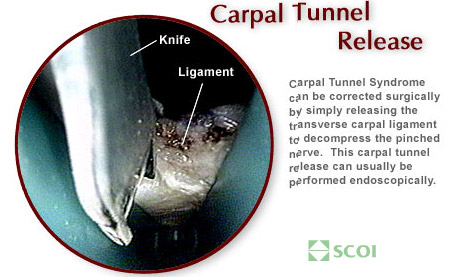
The standard surgical technique for median nerve decompression — that is, carpal tunnel release — has been a very successful operation restoring most patients to their prior activities.
One of the major draw backs to standard, open carpal tunnel release was the slowness of recovery in the palm side surgical scar. Often, the 2 inch palm side scar would remain sensitive to direct pressure for approximately six to eight weeks. in the working patient, this scar sensitivity could preclude return to normal work activities. Recently, orthopedic technology has advanced to the point where a standard arthroscope has been specially modified to be of use in carpal tunnel surgery.
To employ the endoscopic technique in carpal tunnel release, a small 1/2 inch horizontal incision is made at the wrist and the arthroscope is introduced underneath the transverse carpal ligament. A cannula is inserted into the hand, just under the offending ligament. The surgeon looks through a scope and uses a small knife to simply cut the ligament, thus freeing the nerve. A special blade attached to the tip of the arthroscope is then utilized to incise the transverse carpal ligament from the inside of the carpal tunnel. In effect, by cutting through the transverse carpal ligament, the compression on the median nerve is alleviated and the nerve is thus allowed to go on the heal. With nerve healing, the painful wrist syndrome is corrected.
Endoscopic carpal tunnel surgery is performed on an outpatient basis utilizing a local anesthetic to numb the arm. After the procedure, a splint is applied to the wrist and the patient is discharged and allowed to go home. Within a week, the splint is removed, a temporary wrist splint is applied and hand rehabilitation is initiated.
See how easy it is: download a brief QuickTime clip of an Endoscopic Carpal Tunnel Release.